GIAPREZA in septic shock
Stabilize MAP and reduce
vasopressor load
Trial Design
ATHOS-3: A landmark trial in septic shock1-3
GIAPREZA was studied in ATHOS-3, an international, randomized, double-blind, placebo-controlled trial of 321 patients with distributive shock who remained hypotensive despite fluid and vasopressor therapy.1,4
Slide table to view more
Treatment arms1 GIAPREZA (n=163) plus SOC vasopressors*,† Placebo (n=158) plus SOC vasopressors*,† | Primary endpoint1 An increase in MAP at hour 3 of at least 10 mmHg, or a MAP response of ≥75 mmHg, without an increase in baseline vasopressor dosing. |
Secondary endpoints1 - Mean change in cardiovascular SOFA score at hour 48 - Mean change in total SOFA score at hour 48 | |
Select additional endpoint1 All-cause mortality through day 28. |
Slide table to view more
| Select baseline patient characteristics (N=321)1 | GIAPREZA + SOC (n=163) | Placebo + SOC (n=158) |
|---|---|---|
| Median MAP, mmHg (IQR) | 66.3 (63.7-69.0) | 66.3 (63.0-68.3) |
| Median APACHE II score (IQR) | 27 (22-33) | 29 (22-34) |
| Cause of shock, sepsis (%) | 127 (77.9%) | 132 (83.5%) |
| Median vasopressor dose (NED), mcg/kg/min (IQR) | 0.33 (0.23-0.56) | 0.34 (0.23-0.56) |
| Vasopressin use during 6 hours before randomization (%) | 113 (69.3%) | 111 (70.3%) |
*Standard-of-care vasopressors included norepinephrine, epinephrine, dopamine, phenylephrine, and vasopressin.4
†Doses of GIAPREZA or placebo were titrated to a target MAP of ≥75 mmHg during the first 3 hours of treatment while doses of other vasopressors were maintained. From hour 3 to hour 48, GIAPREZA or placebo was titrated to maintain a MAP between 65 and 70 mmHg while reducing doses of other vasopressors.4
MAP Stabilization
3x more patients achieved and sustained target MAP when GIAPREZA was used with SOC1,4
Slide table to view more

Median time to reach target MAP was 5 minutes
Rapid MAP stabilization helps you
quicklydetermine patient response in the ICU1,4
48% of patients who achieved target MAP within 3 hours reached it within the first 30 minutes of treatment at doses ≤5 ng/kg/min5
The effect on MAP was sustained for at least the first 3 hours of treatment4
Powerful MAP results in a broad range of patients
Slide table to view more
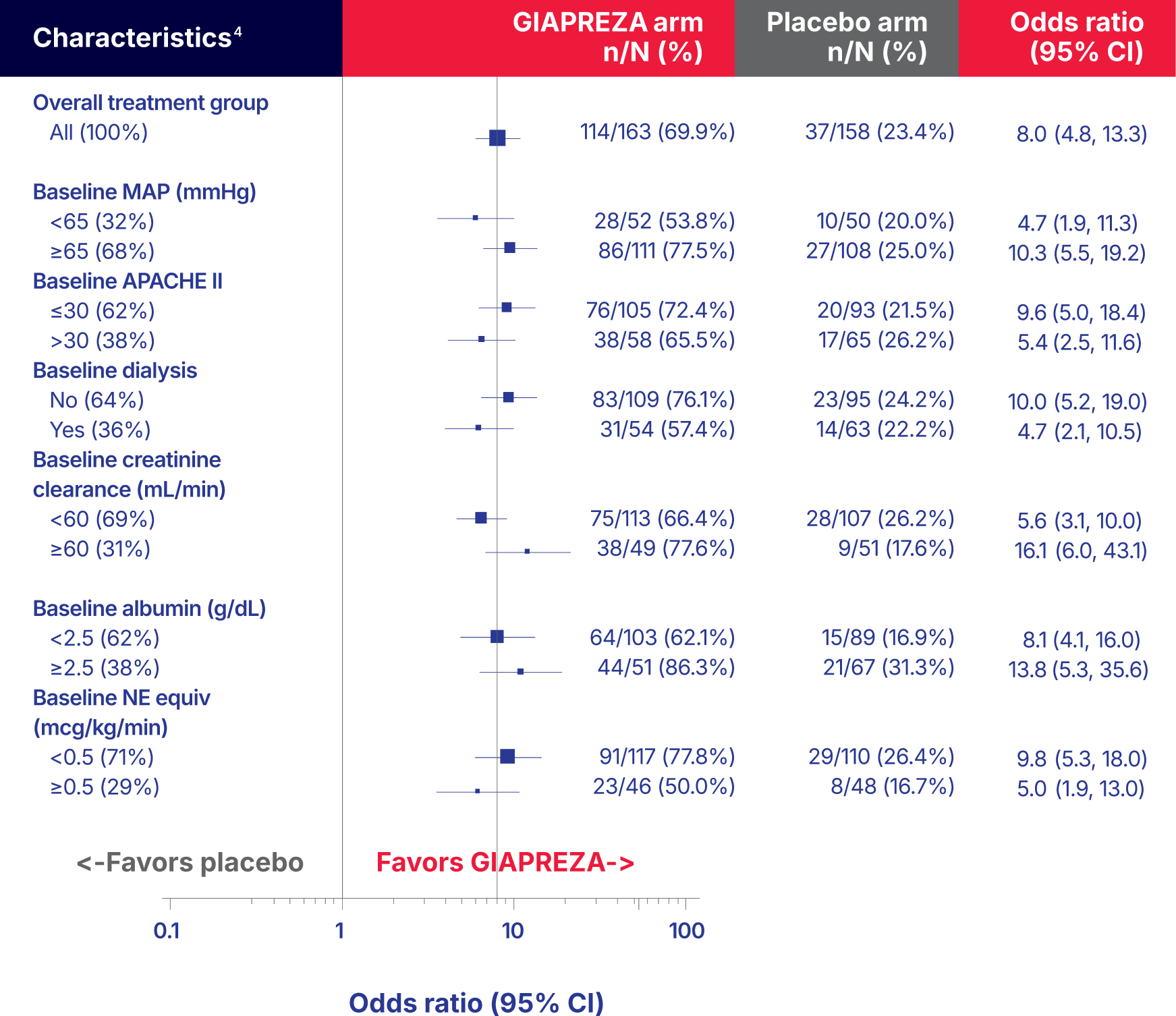
Patients with a history of ACEi and ARB favored GIAPREZA over placebo but interpretation should consider the small sample sizes (9% and 7%, respectively).4
Note: The figure above presents effects in select subgroups, all of which are baseline characteristics. The 95% confidence limits that are shown do not take into account the number of comparisons made and may not reflect the effect of a particular factor after adjustment for all other factors. Apparent homogeneity or heterogeneity among groups should not be overinterpreted.4

Patient Survival
Increased patient survival at day 28 with GIAPREZA + SOC1,6
Slide table to view more

A meta-analysis found no difference in mortality rates between angiotensin II and norepinephrine (46.2% vs 54.2%; RR, 0.85 [95% CI, 0.69-1.06])
-2021 SSC Guidelines7,*
Not statistically significant. Mortality through day 28 was an exploratory endpoint in ATHOS-3. The study was not powered to detect a difference in mortality. There were secondary endpoints not reported on this website.1
*The SSC released updated global guidelines in October 2021 for clinicians caring for adult patients with sepsis or septic shock.7
There was a higher incidence of arterial and venous thrombotic and thromboembolic events in patients who received GIAPREZA compared to placebo-treated patients in the ATHOS-3 study (13% vs 5%).4
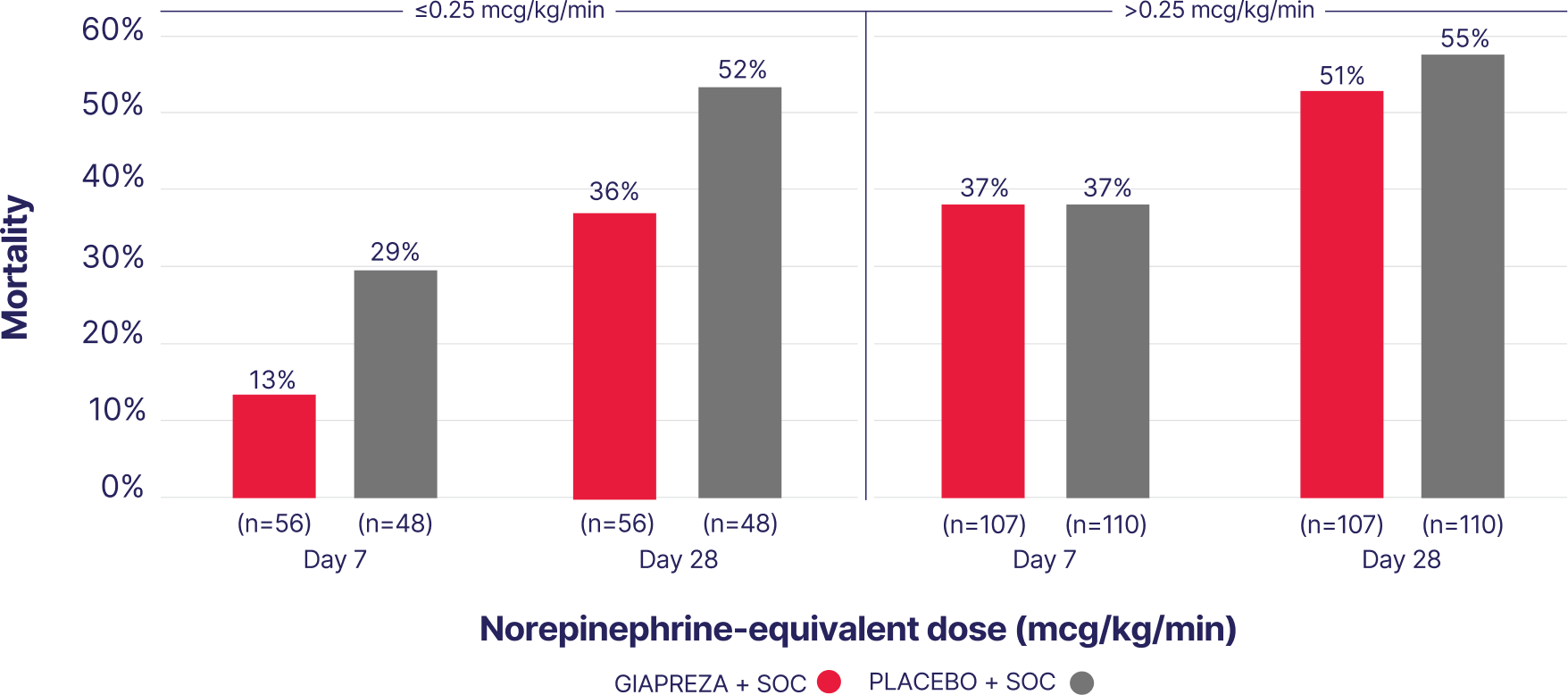
Survival benefit was greatest when
initiated with lower vasopressor doses8
In an exploratory post hoc analysis of ATHOS-3, early use of GIAPREZA plus SOC was associated with improved survival vs placebo plus SOC.8
Slide table to view more
For complete Safety Information of GIAPREZA, .
DON’T WAIT—start GIAPREZA sooner to help reduce mortality and lower doses of other vasopressors.8
VASOPRESSOR LOAD
With GIAPREZA, patients needed lower mean doses of SOC vasopressors1
Slide table to view more

Norepinephrine-equivalent dose (NED) is a standardized way to express the total vasopressor burden a patient is receiving—by converting all vasopressors into an equivalent dose of norepinephrine for comparison.9
Clinical Markers
GIAPREZA: a catecholamine-sparing agent to target RAAS and increase patient survival6,10,11
In an exploratory post hoc analysis of ATHOS-3, a shock-disrupted RAAS pathway was confirmed as a key contributor to low MAP. The analysis uncovered abnormally high renin levels and ANG I/II ratios, suggesting RAAS dysfunction, which correlated with a much higher risk of mortality.10
renin levels10
limit of normal10,*
High renin levels correlated with10:
Slide table to view more
| GIAPREZA effectively reduced renin and ANG I levels for better outcomes10: | GIAPREZA + SOC | Placebo + SOC |
|---|---|---|
| Median reduction in serum renin levels, % | 54.3 | 14.1 |
| Median reduction in serum ANG I levels, % | 39.7 | 7 |
| 28-day mortality, % [median (IQR)]† | 51 (39-65) | 70 (59-80) |
| Ventilator liberation by day 7 (alive and ventilator-free), % [median (IQR)]† | 28 (18-43) | 14 (8-25) |
| RRT liberation by day 7 (alive and RRT free), % [median (IQR)]† | 43 (25-66) | 12 (5-27) |
| ICU discharge by day 28, % [median (IQR)]† | 44 (32-58) | 22 (14-33) |
*The upper limit of normal was defined as 58.78 pg/mL; the median renin level was 172.7 pg/mL.10
†Values represent outcomes in patients who had renin concentrations above the study population median.10
SAFETY
Safety and tolerability vs placebo and SOC in ATHOS-31
Slide table to view more
| GIAPREZA + SOC (n=163) | GIAPREZA + SOC (n=158) | |
|---|---|---|
| Adverse event of any grade, % (n) | 87.1% (142) | 91.8% (145) |
| Adverse event leading to discontinuation, % (n) | 14.1% (23) | 21.5% (34) |
| Any serious adverse event with frequency ≥1% in either study group, % (n) | 60.7% (99) | 67.1% (106) |
Adverse reactions occurring in ≥4% of patients treated with GIAPREZA and ≥1.5% more often than in placebo‑treated patients included thromboembolic events, including arterial and venous thrombosis events (12.9% vs 5.1%), deep vein thrombosis (4.3% vs 0.0%), thrombocytopenia (9.8% vs 7.0%), tachycardia (8.6% vs 5.7%), fungal infection (6.1% vs 1.3%), delirium (5.5% vs 0.6%), acidosis (5.5% vs 0.6%), hyperglycemia (4.3% vs 2.5%), and peripheral ischemia (4.3% vs 2.5%).4
Thromboembolic events
- In ATHOS-3, serious adverse events (SAEs) were reported. The Prescribing Information grouped SAEs and adverse events, including thromboembolic events, as presented under a single category1,4
- The incidence of patients with a grade 3 or 4 (severe or life-threatening) thromboembolic event was 9 (5.5%) events in the GIAPREZA group vs 5 (3.2%) in the placebo group12
- In the GIAPREZA group, 12/25 (48%) thromboembolic events occurred within 5 days of randomization in comparison to 7/8 (87.5%) events in the placebo arm12
Use concurrent venous thromboembolism (VTE) prophylaxis.4
Fewer GIAPREZA-treated patients discontinued treatment vs placebo due to adverse events1
Fewer GIAPREZA-treated patients experienced adverse events and serious adverse events vs placebo1
Slide table to view more

*Instrumental ADL refers to preparing meals, shopping for groceries or clothes, using the telephone, managing money, and other such activities.13
†Self-care ADL refers to bathing, dressing and undressing, feeding self, using the toilet, and taking medications without being bedridden.13
Connect with a GIAPREZA sales
representative for information and support.
ACE=angiotensin-converting enzyme; ACEi=ACE inhibitor; ADL=activities of daily living; ANG=angiotensin; ARB=angiotensin II receptor blocker; APACHE 2=Acute Physiology and Chronic Health Evaluation II; ATHOS-3=Angiotensin II for the Treatment of High-Output Shock; CI=confidence interval; ICU=intensive care unit; IQR=interquartile range; MAP=mean arterial pressure; NE=norepinephrine; NED=NE-equivalent dose; RAAS=renin-angiotensin-aldosterone system; RRT=renal replacement therapy; SOC=standard of care; SOFA=Sequential Organ Failure Assessment; SSC=Surviving Sepsis Campaign.
References:
- Khanna A, English SW, Wang XS, et al. Angiotensin II for the treatment of vasodilatory shock. N Engl J Med. 2017;377(5):419-430. doi:10.1056/NEJMoa1704154
- Andrews L, Benken J, Benedetti E, et al. Effects of angiotensin II in the management of perioperative hypotension in kidney transplant recipients. Clin Transplant. 2022;36(9):e14754. doi:10.1111/ctr.14754
- National Center for Biotechnology Information. PubChem Compound Summary for CID 172198, angiotensin II. Accessed January 14, 2025. https://pubchem.ncbi.nlm.nih.gov/compound/Angiotensin-II-human
- GIAPREZA. Prescribing information. La Jolla Pharmaceutical Company; 2021.
- Ham KR, Boldt DW, McCurdy MT, et al. Sensitivity to angiotensin II dose in patients with vasodilatory shock: a prespecified analysis of the ATHOS-3 trial. Ann Intensive Care. 2019;9(1):63. doi:10.1186/s13613-019-0536-5
- Supplementary appendix to: Khanna A, English SW, Wang XS, et al. Angiotensin II for the treatment of vasodilatory shock. N Engl J Med. 2017;377(5):419-430. doi:10.1056/NEJMoa1704154
- Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181-1247. doi:10.1007/s00134-021-06506-y
- Wieruszewski PM, Bellomo R, Busse LW, et al. Initiating angiotensin II at lower vasopressor doses in vasodilatory shock: an exploratory post‑hoc analysis of the ATHOS-3 clinical trial. Crit Care. 2023;27(1):175. doi:10.1186/s13054-023-04446-1
- Kotani Y, Di Gioia A, Landoni G, et al. An updated "norepinephrine equivalent" score in intensive care as a marker of shock severity. Crit Care. 2023;27(1):29. doi:10.1186/s13054-023-04322-y
- Bellomo R, Forni LG, Busse LW, et al. Renin and survival in patients given angiotensin II for catecholamine-resistant vasodilatory shock. A clinical trial. Am J Respir Crit Care Med. 2020;202(9):1253-1261. doi:10.1164/rccm.201911-2172OC
- Buckley MS, Barletta JF, Smithburger PL, et al. Catecholamine vasopressor support sparing strategies in vasodilatory shock. Pharmacotherapy. 2019;39(3):382-398. doi:10.1002/phar.2199
- Data on File. Innoviva Specialty Therapeutics; 2023.
- Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0. US Department of Health and Human Services, National Institutes of Health, National Cancer Institute. Published May 28, 2009. Updated June 14, 2010. Accessed December 12, 2025. https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf
IMPORTANT SAFETY INFORMATION
Indication
GIAPREZA® (angiotensin II) increases blood pressure in adults with septic or other distributive shock.
Contraindications
None.
Warnings and Precautions
The safety of GIAPREZA was evaluated in 321 adults with septic or other distributive shock in a randomized, double-blind, placebo-controlled study, ATHOS-3. There was a higher incidence of arterial and venous thrombotic and thromboembolic events in patients who received GIAPREZA compared to placebo-treated patients in the ATHOS-3 study (13% vs. 5%). The major imbalance was in deep venous thromboses. Use concurrent venous thromboembolism (VTE) prophylaxis.
Adverse Reactions
The most common adverse reactions reported in greater than 10% of GIAPREZA-treated patients were thromboembolic events. Adverse reactions occurring in ≥4% of patients treated with GIAPREZA and ≥1.5% more often than placebo-treated patients in the ATHOS-3 study were thromboembolic events (including deep vein thrombosis), thrombocytopenia, tachycardia, fungal infection, delirium, acidosis, hyperglycemia, and peripheral ischemia.
Drug Interactions
Angiotensin converting enzyme (ACE) inhibitors may increase response to GIAPREZA. Angiotensin II receptor blockers (ARBs) may reduce response to GIAPREZA.
You are encouraged to report negative side effects of prescription drugs to the FDA.
To report SUSPECTED ADVERSE REACTIONS, please contact:
Before administering, please see the Full Prescribing Information for GIAPREZA.